
The Laboratory Benefit Management (LBM) Program, administered by BeaconLBS, enables health plans to improve the quality of lab testing provided to health plan members. This is accomplished by encouraging providers to use in-network labs, who are held to a higher quality standard comparable to the complexity of testing they offer, so they can be eligible for reimbursement.
Although provider offices may perform some lab testing in-house, with more complex tests, additional expertise, processes, and equipment are generally needed. Lab quality is a vital part of the LBM Program, necessitating this review of essential laboratory requirements for quality.
The LBM quality requirements for labs under this program are:
Electronic Orders and/or Results
Electronic orders and/or results may contribute to the efficiency and safety of laboratory testing by reducing the duplication of test orders and diminishing the risk of misidentification of patient orders. When an order is unclear, inappropriate testing may be performed since the order was interpreted differently than intended. For example, a study in 2015 reviewed the accuracy of manual data-entry handwritten laboratory orders and detected errors in 10% of the orders with 75% of these as transcription errors. These errors may affect overall cost and efficiency. However, when a lab provides electronic ordering capabilities to the provider, data accuracy may be improved and may reduce mistakes so the right test, with no ambiguity, is performed for the right member.
An electronic ordering system may also decrease turnaround times (TAT) and improve accessibility of results Electronic results are generally available sooner because there is no fax or mail delay. Additionally, electronic results may increase the reliability of results. In one study of 459 institutions, the researchers found that 7.1% of telephoned results were incorrectly transmitted to the ordering physician(s). Ensuring accuracy of results will enable the provider to make a clinical judgement and possibly begin needed treatment sooner. In many cases, these results can be electronically received into the member’s medical record as data, instead of a document or image, so the health care team can more easily monitor trends in results over time and perhaps identify clinical issues earlier.
Electronic orders and/or results have the opportunity to provide additional privacy considerations for patients. As many labs offer the ability for patients to access results electronically as well, patients can more easily maintain records of the testing already done. This, in turn, can help to reduce repeat, unnecessary, testing.
CAP/JCAHO Accreditation
For certain complex testing, College of American Pathologists (CAP) or Joint Commission (JCAHO) accreditation is required. When a lab earns either of these, it means that it has been inspected and its quality measures have been reviewed, by an outside impartial expert organization, and found to be appropriate.
Guidelines set forth in the CAP Laboratory Accreditation Program checklists specify that all clinical laboratory testing must essentially meet those requirements defined for high-complexity testing under CLIA-88, including test validation standards, reportable/reference ranges, performance criteria, and proficiency testing. This accreditation may provide ordering providers and members with higher confidence in the accuracy of the test results knowing they were performed by a qualified entity.
Secondary Complex Pathology Reviews and Sub-Specialist Review
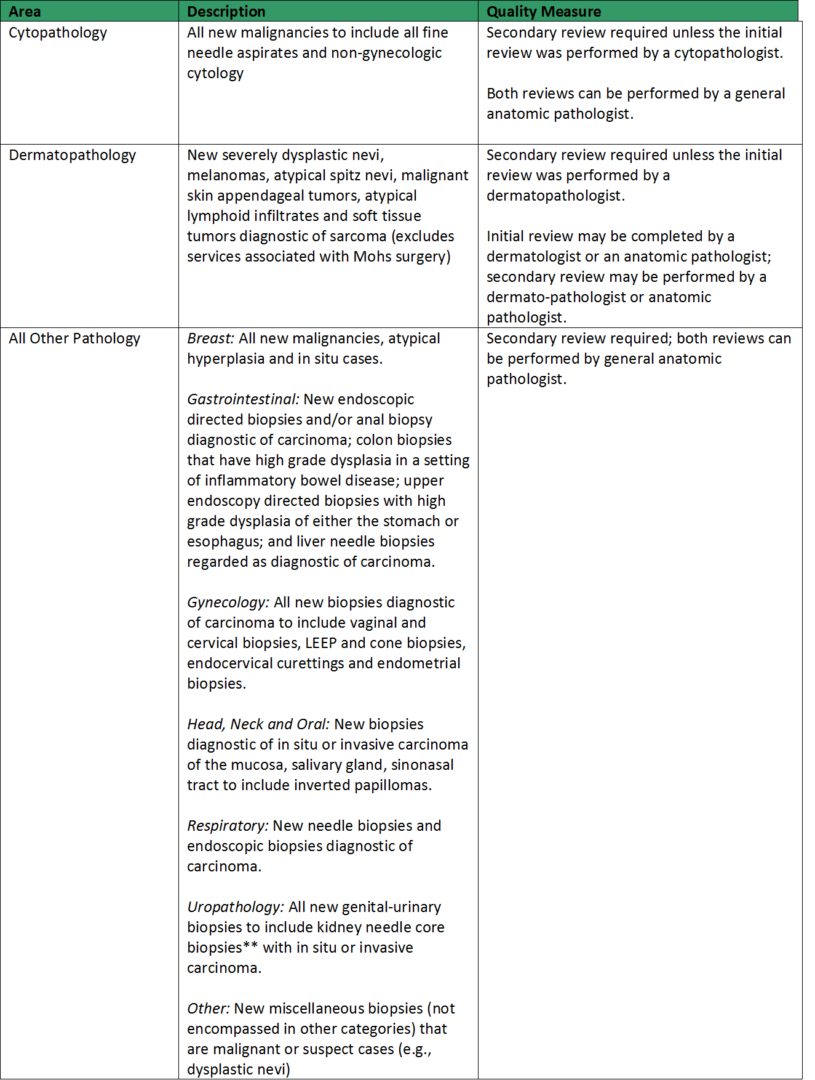
Secondary complex pathology review is a quality measure that applies to anatomic pathology and cytology services (see Table 1). Even in the age of technology, anatomic pathology remains significantly dependent upon an individual physician to perform an interpretation and convey a diagnosis. To meet this requirement, a lab certifies that for certain complex pathology diagnoses, a secondary review will be performed. Secondary complex pathology review can reduce the rates of diagnostic discrepancy and/or variability.
There are multiple studies that have documented the rates of diagnostic discrepancy and/or variability when secondary complex pathology reviews are not performed. A CAP Q-Probes program analyzed the number of anatomic pathology discrepancies from 74 self-reporting laboratories that were prospectively performing secondary review of 100 surgical pathology or cytology specimens. The mean laboratory discrepancy frequency was 6.7% and of those, 5.3% had a moderate or marked effect on patient care. Out of 6,186 specimens, there were 415 discrepancies and in using self-assessment to determine error severity, 16.6% of all errors resulted in some form of patient harm.
Table 1. Secondary Reviews
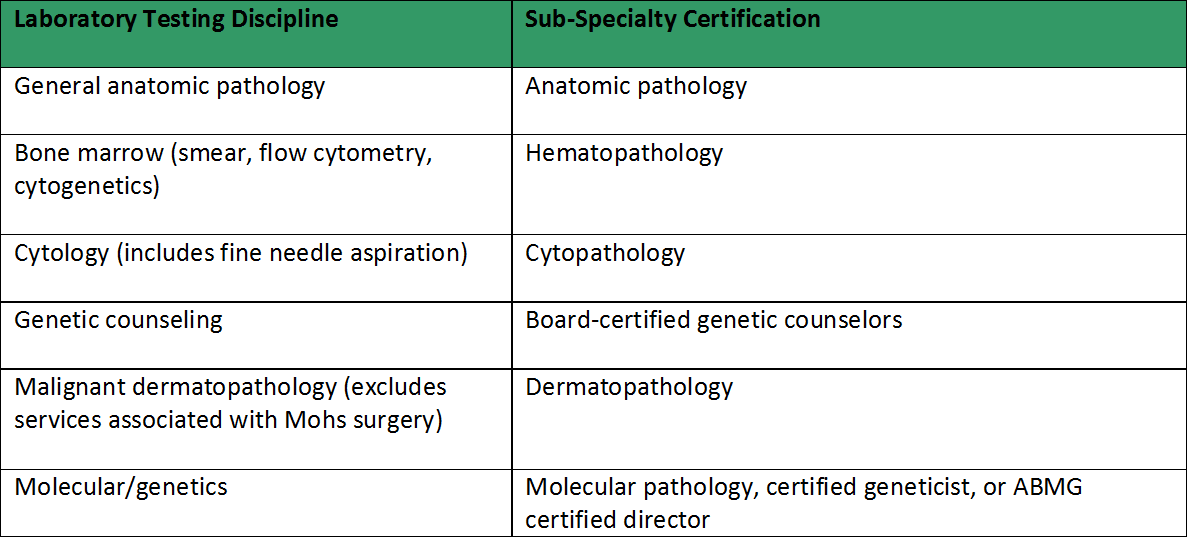
Similar to secondary complex pathology review the sub-specialist quality measure means that the lab certifies that, based on the complexity of the test, and where sub-specialty certification exists, they will have the appropriately subspecialists for test review (see Table 2). This measure stretches beyond anatomic pathology and includes various clinical pathology areas as well.
Many academic centers, in an effort to increase quality and reduce diagnostic inaccuracy, have adopted partial or complete subspecialty pathologist sign-out of cases. Many clinicians accept sub-specialty sign-out as the “gold standard” for review and diagnosis in pathology. For example, the Department of Pathology at the University of Pittsburgh Medical Center uses a subspecialty-based practice model, in which separate “Centers of Excellence” (COEs) take responsibility for cases from different organ systems, including thoracic, gastrointestinal, bone and soft tissue, head and neck, genitourinary, neurologic, and transplant pathology.
As the field of medical genetics is rapidly expanding, there are specific areas of expertise that are important components of the clinical genetics health care delivery system. The subspecialty areas of Cytogenetics, Molecular Genetics, and HLA testing fall under Clinical Pathology. While there are few published studies on the topic of these clinical pathology programs and subspecialty review, there are several guidelines from professional societies or task forces that highlight subspecialty certification or accreditation.
A Task Force on Genetic Testing was created by the National Institutes of Health – Department of Energy Working Group on the Ethical, Legal, and Social Implications of Human Genome Research. This Task Force recommends “that for laboratories performing high complexity tests in the proposed specialty of molecular genetics, as well as in biochemical genetics and cytogenetics, personnel serving as directors or technical supervisors must have formal training in human and medical genetics, as documented by holding certification from an organization that assesses knowledge of human and medical genetics as part of its certification process, such as the American Board of Medical Genetics”.
Where two specially trained providers discuss and agree on a diagnosis, patients and their families may have a higher confidence that the diagnosis is accurate and that the care provider will be better equipped to determine and implement the appropriate treatment. Labs that meet these standards certify that two anatomic pathologists, or a pathologist specially trained in specific sub-specialties, will perform the test reviews.
Table 2. Sub-Specialist Disciplines
Conclusion
For the LBM program, BeaconLBS maintains in its Physician Decision Support ® (PDS) platform, a database of the quality of in-network labs. The PDS makes this information available to ordering provider teams, at the point of care, so that the provider can make informed decisions prior to the lab order being placed. For laboratories that meet the quality criteria discussed in this article, the Lab Benefit Management Program encourages higher reliability of test results outcomes and lower out-of-pocket costs for members.
References:
- Delvaux et al. Implementation Science (2017) 12:147, DOI 10.1186/s 13012-017-0685-6
- Seabrook JM, Hubbard RA. Achieving quality reproducible results and maintaining compliance in molecular diagnostic testing of Human Papillomavirus. Arch Pathol Lab Med. 2003;127:978-983
- Dahl J. “Quality, Assurance, Diagnosis, Treatment, and Patient Care.” Patient Safety and Quality Healthcare. Available at: http://www.psqh.com/marapr06/pathologist.html (Accessed: March 1, 2018).
- Schifman RB, Steindel SJ, Howanitz PJ. Quality of telephone support by clinical laboratories: a College of American Pathologists Q-Probes study involving 459 institutions. Am J Clin Pathol. 1996;105:517A-518A.
- Raab SS, Nakhleh RE, Ruby SG. Patient safety in anatomic pathology. Measuring discrepancy frequencies and causes. Arch Pathol Lab Med. 2005;129:459-466.
- Georgiou A, Westbrook J. Computerized order entry systems and pathology services – A synthesis of the evidence. Clin Biochem Rev. 2006;27:79-87
- Vecellio E, Malley MW, Toouli G, et al. Data quality associated with handwritten laboratory test requests: classification and frequency of data-entry errors for outpatient serology tests. Health Inf Manag. 2015;44(3):7-12. Holtzman NA, Watson MS (eds). “Final Report of the Task Force on Genetic Testing.” National Institutes of Health. 1997. Available at: http://www.genome.gov/10002403 (Accessed: March 1, 2018).